Class 3 malocclusion Causes, Diagnosis, and Treatment Options
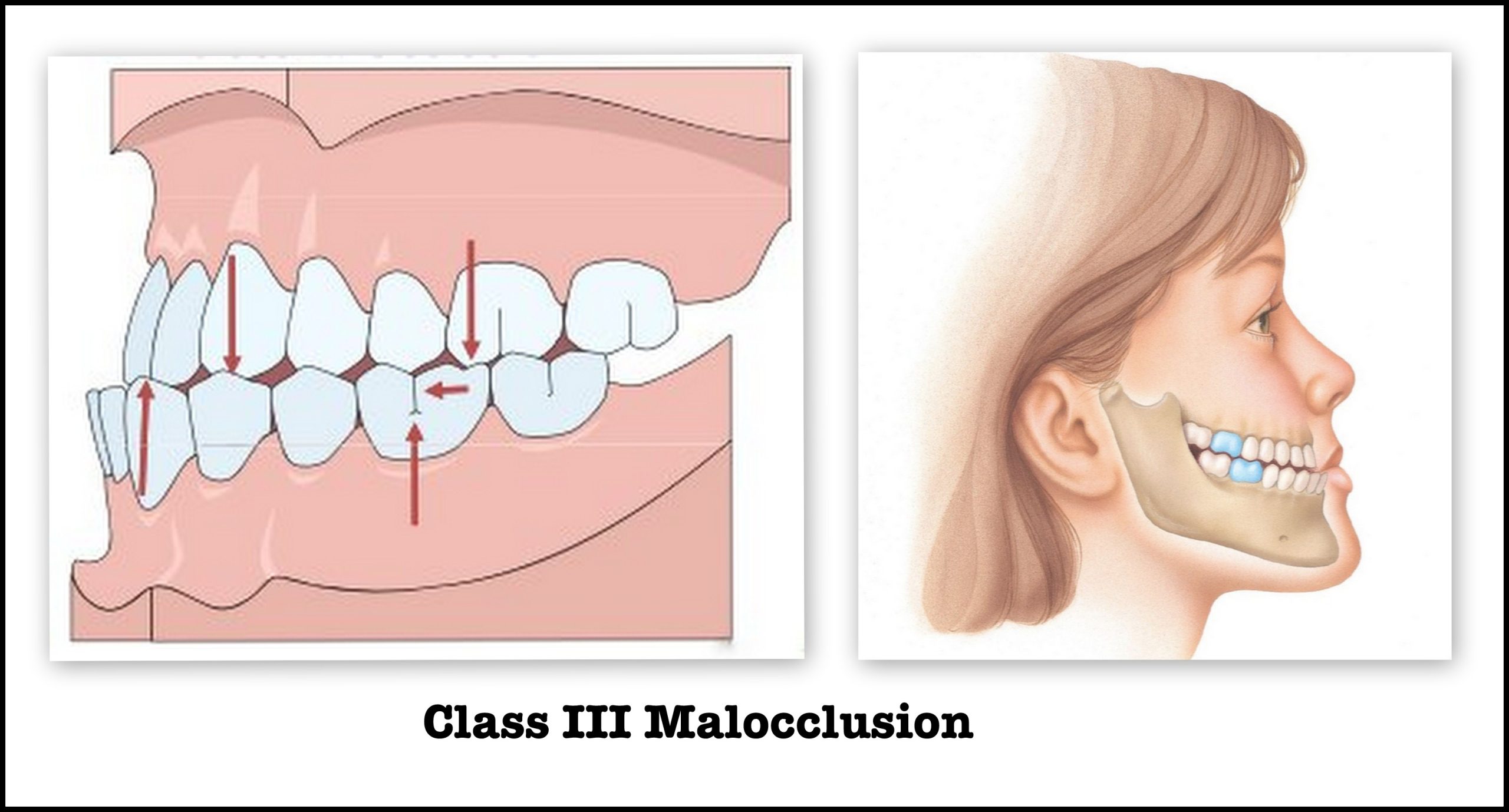
Class III malocclusion, commonly referred to as an underbite, is a dental condition characterized by the lower teeth protruding beyond the upper teeth. This misalignment can affect not only the aesthetic appearance of a person’s smile but also their oral function, health, and overall quality of life. Understanding the intricacies of Class III malocclusion, its causes, diagnosis, and treatment options, is essential for both dental professionals and patients seeking to address this condition effectively.
What is Class 3 Malocclusion?
Class III malocclusion occurs when the lower jaw (mandible) is positioned forward relative to the upper jaw (maxilla), resulting in an underbite. This misalignment can be skeletal, dental, or a combination of both. In skeletal Class III malocclusion, the discrepancy is due to the relative positions or sizes of the jawbones, whereas in dental Class 3 malocclusion, the teeth themselves are misaligned.
Class 3 malocclusion can vary in severity, from mild cases where the lower teeth slightly overlap the upper teeth, to severe cases where the entire lower jaw is markedly forward. This condition not only affects the bite and chewing efficiency but can also impact speech, facial appearance, and self-esteem.
Causes of Class 3 Malocclusion
The development of Class 3 malocclusion can be attributed to various factors, including genetic, environmental, and developmental influences. Understanding these causes can help in formulating appropriate treatment plans.
- Genetic Factors:
- Hereditary Traits: Genetics play a significant role in the development of Class III malocclusion. If one or both parents have this condition, there is a higher likelihood that their offspring may inherit it. This hereditary predisposition can influence the size and shape of the jaws and teeth alignment.
- Syndromes and Genetic Disorders: Certain genetic syndromes, such as Crouzon syndrome and Treacher Collins syndrome, can predispose individuals to Class 3 malocclusion due to craniofacial anomalies.
- Environmental Factors:
- Thumb Sucking and Prolonged Pacifier Use: Habitual thumb sucking or extended use of pacifiers beyond the age of three can affect jaw development and alignment, contributing to malocclusion.
- Mouth Breathing: Chronic mouth breathing, often due to nasal obstructions or allergies, can alter the natural growth patterns of the jaws and dental arches.
- Developmental Factors:
- Differential Jaw Growth: Discrepancies in the growth rates of the upper and lower jaws can lead to Class III malocclusion. Rapid growth of the mandible or insufficient growth of the maxilla can result in an underbite.
- Early Loss of Baby Teeth: Premature loss of primary (baby) teeth can disrupt the alignment of permanent teeth, potentially leading to malocclusion.
Diagnosis of Class III Malocclusion
Accurate diagnosis of Class III malocclusion is crucial for determining the most effective treatment approach. A comprehensive diagnostic process involves several steps, including clinical examination, radiographic evaluation, and the use of diagnostic models.
- Clinical Examination:
- Visual Assessment: A dentist or orthodontist will visually inspect the patient’s facial profile, jaw alignment, and teeth occlusion. The presence of an underbite, crossbite, or other dental abnormalities will be noted.
- Functional Evaluation: The clinician will assess the patient’s bite function, chewing efficiency, and speech. Any functional impairments related to malocclusion will be documented.
- Radiographic Evaluation:
- Panoramic X-rays: Panoramic radiographs provide a broad view of the upper and lower jaws, allowing for the assessment of jawbone structure, tooth alignment, and the presence of impacted or missing teeth.
- Cephalometric Analysis: Cephalometric radiographs are essential for evaluating the skeletal relationships between the jaws and the cranial base. This analysis helps in determining whether the malocclusion is primarily skeletal or dental in nature.
- Cone Beam Computed Tomography (CBCT): CBCT scans offer three-dimensional imaging, providing detailed information about the bone structure, tooth positions, and soft tissues. This advanced imaging technique is particularly useful for complex cases.
- Diagnostic Models:
- Dental Impressions: Dental impressions of the patient’s teeth are taken to create accurate models of the upper and lower arches. These models are used to study the occlusion, plan treatment strategies, and fabricate orthodontic appliances.
Treatment Options for Class III Malocclusion
The treatment of Class III malocclusion depends on the severity of the condition, the patient’s age, and whether the malocclusion is primarily skeletal or dental. Treatment options range from orthodontic interventions to surgical correction, often requiring a multidisciplinary approach involving orthodontists, oral surgeons, and other dental specialists.
- Orthodontic Treatment:
- Braces: Traditional braces, consisting of brackets and wires, are commonly used to correct dental malocclusions. They apply continuous pressure to move the teeth into proper alignment. For mild to moderate Class III malocclusion, braces can help reposition the teeth and improve the bite.
- Clear Aligners: Clear aligners, such as Invisalign, offer a more aesthetic alternative to braces. These removable, transparent trays gradually shift the teeth into their desired positions. Clear aligners are suitable for mild to moderate cases and require strict patient compliance.
- Functional Appliances: Functional appliances, such as reverse pull headgear or face masks, are used to modify jaw growth in growing children. These appliances apply forward traction to the maxilla, encouraging its growth and improving the jaw relationship.
- Orthopedic Treatment:
- Rapid Maxillary Expansion (RME): RME is a technique used to widen the upper jaw in growing children. A special device called a palatal expander is placed on the upper teeth and gradually widened over time. This procedure can help correct crossbites and improve the overall alignment of the jaws.
- Surgical Treatment:
- Orthognathic Surgery: In severe cases of Class III malocclusion, where there is a significant skeletal discrepancy, orthognathic surgery may be necessary. This surgical procedure involves repositioning the jaws to achieve proper alignment. It is often combined with orthodontic treatment to ensure optimal results.
- Genioplasty: Genioplasty is a surgical procedure that involves reshaping or repositioning the chin to improve facial balance and aesthetics. It can be performed in conjunction with orthognathic surgery or as a standalone procedure.
- Combination Treatment:
- Orthodontics and Surgery: For severe Class III malocclusion, a combination of orthodontic treatment and orthognathic surgery is often the most effective approach. Orthodontic appliances are used to align the teeth before surgery, and post-surgical orthodontics fine-tunes the occlusion.
- Growth Modification:
- Timing of Treatment: Early intervention during the growth phase can be beneficial for children with Class III malocclusion. Growth modification techniques, such as the use of functional appliances and orthopedic devices, can guide jaw growth and improve the jaw relationship.
Impact of Untreated Class III Malocclusion
Leaving Class III malocclusion untreated can have significant consequences on oral health, function, and overall well-being. The potential impacts of untreated malocclusion include:
- Dental Health Issues:
- Tooth Wear and Damage: The misalignment of the teeth can lead to uneven wear and tear on the enamel, increasing the risk of tooth decay and damage.
- Periodontal Problems: Malocclusion can contribute to gum recession, periodontal disease, and other oral health issues due to difficulty in maintaining proper oral hygiene.
- Functional Impairments:
- Chewing and Digestion: An improper bite can affect the efficiency of chewing, leading to digestive problems and nutritional deficiencies.
- Speech Difficulties: Malocclusion can impact speech articulation, causing difficulties in pronouncing certain sounds and affecting overall speech clarity.
- Aesthetic Concerns:
- Facial Appearance: Class III malocclusion can alter the facial profile, leading to an unbalanced or asymmetrical appearance. This can affect self-esteem and confidence.
- Social and Psychological Impact: The aesthetic and functional consequences of malocclusion can have a significant psychological impact, particularly in children and adolescents. Social interactions, self-image, and overall quality of life may be negatively affected.
Preventive Measures and Long-Term Management
While genetic factors contributing to Class III malocclusion cannot be prevented, certain measures can help mitigate the risk and manage the condition effectively.
- Early Dental Visits: Regular dental check-ups from an early age can help in identifying and addressing dental issues promptly. Early detection of malocclusion allows for timely intervention and better outcomes.
- Habit Control: Discouraging harmful oral habits, such as thumb sucking and prolonged pacifier use, can reduce the risk of developing malocclusion. Parents should encourage proper oral hygiene practices and monitor their child’s dental development.
- Orthodontic Evaluation: Children should undergo orthodontic evaluation by the age of seven, as recommended by the American Association of Orthodontists. Early assessment allows for the identification of potential issues and the implementation of growth modification techniques if needed.
- Compliance with Treatment: Patients undergoing orthodontic or orthopedic treatment should adhere to the prescribed regimen and follow the instructions provided by their dental professionals. Consistent compliance is essential for achieving optimal results.
- Maintenance and Retention: After completing orthodontic treatment, the use of retainers is crucial to maintain the corrected alignment of the teeth. Regular follow-up visits with the orthodontist ensure long-term stability and prevent relapse.
Conclusion
Class III malocclusion, characterized by the forward positioning of the lower jaw relative to the upper jaw, can have significant implications for oral health, function, and aesthetics. Understanding the causes, diagnosis, and treatment options for this condition is essential for dental professionals and patients alike.
Effective management of Class III malocclusion requires a comprehensive approach, often involving a combination of orthodontic, orthopedic, and surgical interventions. Early diagnosis and intervention are key to achieving the best outcomes and preventing long-term complications. By addressing Class III malocclusion proactively, individuals can enjoy improved oral health, enhanced facial aesthetics, and a better quality of life.
Related to read:
Best Oral Hygiene Practices For Optimum Oral Health.
How to Whiten Teeth Naturally?
How to keep your gums healthy and disease-free?
References
To ensure the information provided is accurate and up-to-date, the following sources were referenced:
- American Dental Association. (n.d.). Plaque and Tartar. Retrieved from ADA website
- Mayo Clinic. (n.d.). Dental Plaque. Retrieved from Mayo Clinic website
- National Institute of Dental and Craniofacial Research. (n.d.). Periodontal (Gum) Disease. Retrieved from NIDCR website
What are the Features of Angle’s Class III Malocclusion?
Angle’s Class III malocclusion, often referred to as an underbite, is a type of dental misalignment where the lower teeth and jaw project forward beyond the upper teeth and jaw. This condition can be identified by several distinct features:
- Mandibular Protrusion:
- The lower jaw (mandible) is positioned forward relative to the upper jaw (maxilla), leading to a pronounced lower facial profile.
- This can result in a concave facial profile when viewed from the side.
- Dental Misalignment:
- The lower front teeth (incisors) overlap the upper front teeth, creating a negative overjet.
- There may be crowding of the lower teeth due to the forward position of the mandible.
- Occlusal Discrepancies:
- There is often a reverse overbite where the lower front teeth are in front of the upper front teeth when the jaws are closed.
- The posterior teeth (molars and premolars) may also have an abnormal relationship, with the lower teeth positioned ahead of the upper teeth.
- Functional Issues:
- Difficulty in chewing and biting efficiently due to the misalignment of the teeth.
- Speech difficulties, particularly with sounds that require the proper alignment of the teeth and jaws.
- Aesthetic Concerns:
- A more prominent chin and a concave facial profile can affect the overall appearance.
- The smile may appear unbalanced, which can impact self-esteem and social interactions.
- Associated Conditions:
- Class III malocclusion can be associated with temporomandibular joint (TMJ) disorders due to the strain on the jaw joints.
- It can also lead to periodontal issues and increased wear on the teeth due to improper alignment.
Can Class III Malocclusion Be Corrected?
Yes, Class III malocclusion can be corrected through various treatment options depending on the severity of the condition and the patient’s age. The goal of treatment is to achieve proper alignment of the teeth and jaws, improve function, and enhance facial aesthetics. Here are the main treatment approaches:
- Orthodontic Treatment:
- Braces: Traditional metal braces or ceramic braces can be used to move the teeth into proper alignment. This is often the first line of treatment for dental Class III malocclusion.
- Clear Aligners: Clear aligners, like Invisalign, are an alternative to braces for less severe cases. These aligners gradually shift the teeth into the desired position.
- Functional Appliances: In growing children, functional appliances such as reverse pull headgear or facemasks can be used to encourage forward growth of the upper jaw and redirect the growth of the lower jaw.
- Orthopedic Treatment:
- Rapid Maxillary Expansion (RME): This technique involves widening the upper jaw using a palatal expander, which can help correct crossbites and improve overall jaw alignment.
- Surgical Treatment:
- Orthognathic Surgery: For severe skeletal Class III malocclusion in adults, orthognathic surgery may be necessary. This involves repositioning the jaws to achieve proper alignment. The surgery is often combined with orthodontic treatment for optimal results.
- Genioplasty: This surgical procedure reshapes or repositions the chin to improve facial balance and aesthetics. It can be done in conjunction with orthognathic surgery or as a standalone procedure.
- Combination Treatment:
- Orthodontics and Surgery: In many cases, a combination of orthodontic treatment and orthognathic surgery provides the best results. Orthodontic treatment is used to align the teeth before surgery, and post-surgical orthodontics fine-tunes the occlusion.
- Growth Modification:
- Early Intervention: For children, early intervention with functional appliances and orthopedic devices can guide jaw growth and prevent the progression of Class III malocclusion.
What is the Difference Between True and Pseudo Class III Malocclusion?
Class III malocclusion can be categorized into two types: true Class III malocclusion and pseudo (or false) Class III malocclusion. Understanding the differences between these types is crucial for accurate diagnosis and appropriate treatment planning.
- True Class III Malocclusion:
- Skeletal Origin: True Class III malocclusion is primarily due to a skeletal discrepancy between the upper and lower jaws. The mandible is positioned forward relative to the maxilla, leading to a pronounced underbite.
- Genetic Factors: It is often hereditary and can be associated with genetic syndromes affecting craniofacial development.
- Permanent Condition: Without intervention, true Class III malocclusion does not self-correct and usually requires a combination of orthodontic and surgical treatment to achieve proper alignment.
- Jaw Growth: In true Class III malocclusion, the lower jaw may exhibit excessive growth, or the upper jaw may have deficient growth, or a combination of both.
- Pseudo Class III Malocclusion:
- Dental Origin: Pseudo Class III malocclusion is primarily due to dental factors rather than skeletal discrepancies. It results from an abnormal bite pattern or occlusal interferences that cause the lower jaw to shift forward when the teeth are brought together.
- Reversible: Unlike true Class III malocclusion, pseudo Class III malocclusion can often be corrected with orthodontic treatment alone, without the need for surgery. It may involve adjusting the bite and aligning the teeth properly.
- Functional Shift: Patients with pseudo Class III malocclusion typically have a normal jaw relationship at rest, but the lower jaw shifts forward during occlusion due to premature contact of the teeth.
- Early Intervention: Early orthodontic intervention can often correct pseudo Class III malocclusion by eliminating occlusal interferences and guiding the teeth into proper alignment.
What is the Most Common Cause of Class III Malocclusion?
The most common cause of Class III malocclusion is a combination of genetic and environmental factors. However, genetics play a predominant role in the development of this condition. Here are the key causes:
- Genetic Factors:
- Hereditary Traits: A strong genetic component influences the development of Class III malocclusion. If one or both parents have this condition, their children are more likely to inherit it. Genetic predisposition affects the size, shape, and growth patterns of the jaws.
- Craniofacial Syndromes: Certain genetic syndromes, such as Crouzon syndrome and Treacher Collins syndrome, are associated with craniofacial abnormalities that can lead to Class III malocclusion. These syndromes often involve underdevelopment of the maxilla or overdevelopment of the mandible.
- Environmental Factors:
- Thumb Sucking and Prolonged Pacifier Use: These habits can exert pressure on the developing jaws and teeth, potentially contributing to malocclusion. However, they are more commonly associated with Class II malocclusion (overbite).
- Mouth Breathing: Chronic mouth breathing due to nasal obstructions or allergies can influence jaw development and alignment, although its impact is more pronounced on other types of malocclusion.
- Developmental Factors:
- Differential Jaw Growth: A key factor in Class III malocclusion is the differential growth rates of the upper and lower jaws. Excessive growth of the mandible or insufficient growth of the maxilla can result in an underbite.
- Early Loss of Primary Teeth: Premature loss of baby teeth can disrupt the alignment of permanent teeth and contribute to malocclusion.
- Other Contributing Factors:
- Trauma or Injury: Facial trauma or injury to the jaws during development can affect jaw growth and alignment, potentially leading to Class III malocclusion.
- Medical Conditions: Certain medical conditions and congenital anomalies affecting craniofacial development can also contribute to the development of Class III malocclusion.
Understanding the multifactorial nature of Class III malocclusion is essential for developing effective treatment strategies and preventing potential complications. Early diagnosis and intervention can help mitigate the impact of these factors and achieve optimal outcomes for patients.







